Featured Case - Spring 2020
Contributed by Meghana Raghavan MD, Sara Frey MD, Zubeda Sheikh MD, Department of Neurology, West Virginia University School of Medicine
Clinical Presentation
35-year-old woman with a history of mild intellectual disability and epilepsy onset at age 7 was seen in neurology clinic for initial evaluation. She had prolonged episodes of decreased responsiveness when she would be “in a fog” lasting 1-2 days, and at other times would have multiple daily eye rolling episodes as a child. She was started on valproic acid after an EEG showed generalized epileptiform abnormalities. At age 17, she had two convulsions on attempted medication taper. She presented to us at age 35 with a pre-existing diagnosis of Jeavon’s syndrome. Family reported no spells in past several years on continued valproic acid use. An ambulatory EEG was obtained to evaluate for unrecognized seizures and assess interictal burden.
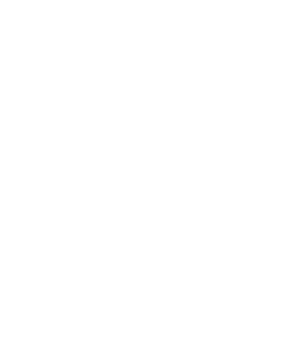
Fig 1 (Bipolar Montage)

Fig 1 (Referential Montage)

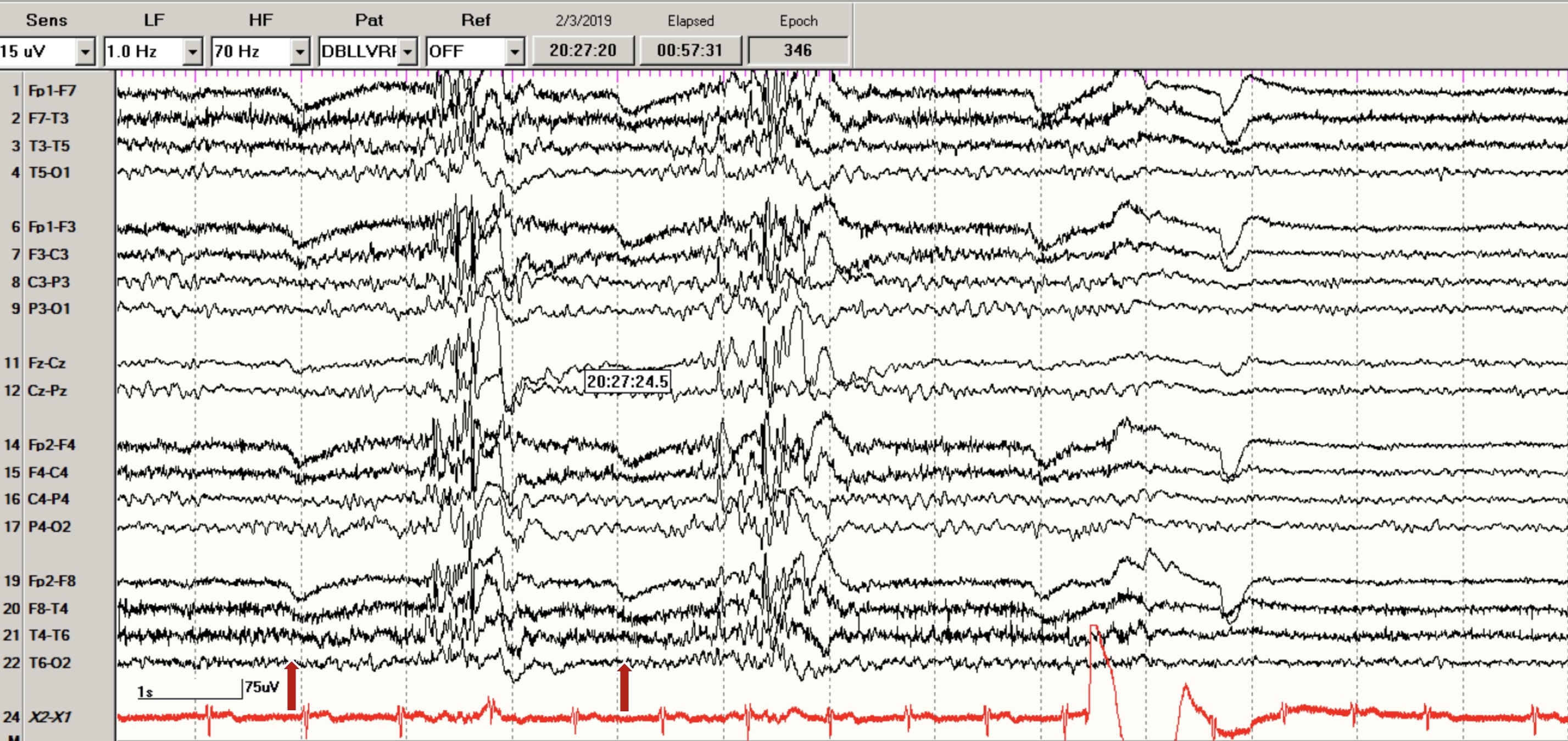
Fig 2 (Bipolar Montage)

Fig 2 (Referential Montage)

Question 1: What phenomenon do the above EEG clips depict?
- Photoparoxysmal response
- Photomyoclonic response
- Eye Closure Sensitivity
- Fixation-off Sensitivity
Answer: (click here)
A1: Correct answer: D. Fixation-off Sensitivity
Fig 1:

Fig 2:

Fig 1 and 2: EEG showing bi-occipital repetitive spikes/polyspikes at 12-16 Hz; at times leading to generalized spike/polyspike wave discharges precipitated by eye closing (shown in red arrows) and disappearing with eye opening (green arrow) and lasting through the duration of eye closure (6 seconds in Fig 2)
The above EEG depicts a phenomenon, most consistent with fixation-off sensitivity (FOS). FOS is characterized by posterior or generalized epileptiform discharges that consistently occur after closing of eyes and last as long as the eyes are closed1,2. This should be differentiated from epileptiform discharges triggered by eye closure (Table 1), which refers to eye closure sensitivity (ECS)2. Epileptiform discharges in ECS occur within 1-3 s after the positive deflection of the eye closure and are typically associated with photosensitivity. Unlike FOS discharges, eye closure related paroxysms are self-limited, of brief duration (lasting 1-4 s, not for entire duration of longer eye-closed periods) and are suppressed by complete darkness. EEG recording during longer periods of eye closure and use of Frenzel lenses (which suppress fixation but do not block retinal stimulation by light) can differentiate FOS from ECS3. The epileptiform discharges of FOS would last for the entire duration of eye closure and would be elicited by use of Frenzel lenses. These tests were not performed on this patient but a 6 second period of generalized epileptiform discharges triggered by eye closing, starting immediately with positive eye deflection and lasting until eye opening as shown in Fig 2 favors FOS over ECS.
Table 1: Clinical and EEG features distinguishing fixation-off and eye closure sensitivity phenomena
| |
Fixation-off sensitivity |
Eye closure sensitivity |
| Trigger |
Elimination of central vision and fixation (by eye closure or use of Frenzel lenses) |
After eye closure |
| Latency |
Start immediately after eye closure |
Occur 1-3 seconds after positive deflection of eye closure |
| Duration |
Lasts as long as eyes remain closed |
Brief and self-limiting Last only for 1-4 seconds |
| Elicited by Frenzel lenses |
Yes |
No |
Question 2: What clinical conditions are the above EEG findings associated with?
- Idiopathic Childhood Occipital Epilepsies
- Idiopathic Generalized Epilepsy
- Asymptomatic children without epilepsy
- All the above
Answer: (click here)
A2: Correct answer: D. All the above
FOS phenomenon is most commonly seen in patients with idiopathic childhood epilepsies with occipital paroxysms, however these may also be seen in symptomatic or cryptogenic focal and generalized epilepsies1. In focal epilepsies, this has been described in Sturge-Weber syndrome4 and focal cortical dysplasia5. FOS has also been reported in asymptomatic non-epileptic children1 (Table 2)
A rare but distinct form of FOS, cryptogenic generalized epilepsy has been described in women with mild intellectual disability with frequent eyelid myoclonia (with or without atypical absences), absence status epilepticus (preferentially catamenial) and generalized tonic clonic seizures6. FOS related EEG features consist mainly of diffuse alpha-like rhythms mixed with bisynchronous sharp and spike/polyspike, often associated with overt clinical manifestations. These patients are not photosensitive and differ from Jeavon’s syndrome (eyelid myoclonia with absences). Jeavon’s syndrome is characterized by eyelid myoclonia with absences, eye closure sensitivity and photosensitivity. Based on our patient’s clinical and EEG phenotype, she is more likely to have FOS related cryptogenic generalized epilepsy with absence status, although we cannot exclude Jeavon’s syndrome as photosensitivity was not tested, nor was ECS ruled out by use of Frenzel lenses. Apart from Jeavon’s syndrome, ECS is seen in juvenile myoclonic epilepsy, childhood and juvenile absence epilepsies and idiopathic occipital epilepsy.
Table 2:
| |
Fixation-off sensitivity |
Eye closure sensitivity |
| Trigger |
Elimination of central vision and fixation (by eye closure or use of Frenzel lenses) |
After eye closure |
| Latency |
Start immediately after eye closure |
Occur 1-3 seconds after positive deflection of eye closure |
| Duration |
Lasts as long as eyes remain closed |
Brief and self-limiting Last only for 1-4 seconds |
| Elicited by Frenzel lenses |
Yes |
No |
| Conditions Associated with EEG finding |
Idiopathic childhood epilepsies with occipital paroxysms Sturge Weber syndrome Focal cortical dysplasia Cryptogenic generalized epilepsy Asymptomatic children without epilepsy |
Jeavon’s syndrome (eyelid myoclonia with absences) Juvenile myoclonic epilepsy Childhood and Juvenile absence epilepsies Idiopathic occipital epilepsy |
Shown below (Fig 3) is an example of ECS in a 17-year-old patient with Juvenile Myoclonic Epilepsy diagnosed at age 15. EEG shows generalized bursts of spike/polyspike wave discharges with onset in 1-2 seconds from eye closure artifact (Fig 3) and last about 1 sec in duration, not for the entire duration of eye closure.
Fig 3: (Bipolar Montage)

Fig 3: (Referential Montage)

A2: Correct answer: C. Acetazolamide
Patients with Hypokalemic Periodic Paralysis can be treated with acetazolamide, a potassium-sparing diuretic; those with CA-channel mutations are more likely to benefit than those with Na-channel mutations. Patients with Hypokalemic Periodic Paralysis should also avoid triggers, such as alcohol and carbohydrate-rich or salty meals. Acute attacks of weakness can be treated with oral potassium salts every 30 minutes until strength improves. Hypokalemic Periodic Paralysis may be allelic to malignant hyperthermia, hence patients undergoing surgery should be monitored accordingly
References
- Brigo F, Rossini F, Stefani A, et al. Fixation-off sensitivity. Clin Neurophysiol 2013;124:221-7.
- Panayiotopoulos CP. Fixation-off, scotosensitive, and other visual-related epilepsies. Adv Neurol 1998;75:139-57.
- Ogura K, Maegaki Y, Koeda T. EEG evaluation of fixation-off sensitivity in eyelid myoclonia with absences. Pediatr Neurol 2005;33:142-5.
- Maher J, Ronen GM, Ogunyemi AO, Goulden KJ. Occipital paroxysmal discharges suppressed by eye opening: variability in clinical and seizure manifestations in childhood. Epilepsia 1995;36:52-7.
- Koutroumanidis M, Tsatsou K, Sanders S, et al. Fixation-off sensitivity in epilepsies other than the idiopathic epilepsies of childhood with occipital paroxysms: a 12-year clinical-video EEG study. Epileptic Disord 2009;11:20-36
- Agathonikou A, Koutroumanidis M, Panayiotopoulos CP. Fixation-off-sensitive epilepsy with absences and absence status: video-EEG documentation. Neurology 1997;48:231-4.